
If WDTC is to recur, there should be objective evidence of this on imaging or Thyroglobulin (Tg) levels in the blood within 5 years following completion of treatment.
Where did the recurrence of cancer come from?
Locoregional recurrence means thyroid cancer that has persisted or recurred in the ‘thyroid bed’ where the thyroid used to be (‘locally’ in the central neck compartment) or anywhere nearby in the neck (‘regionally’ in the lateral neck compartment) – in both cases this would mean cancer that has spread to a lymph node(s) in the neck.
Distant metastatic disease means thyroid cancer that has spread distantly away from the neck (e.g. lungs, bone, liver, brain, etc.).
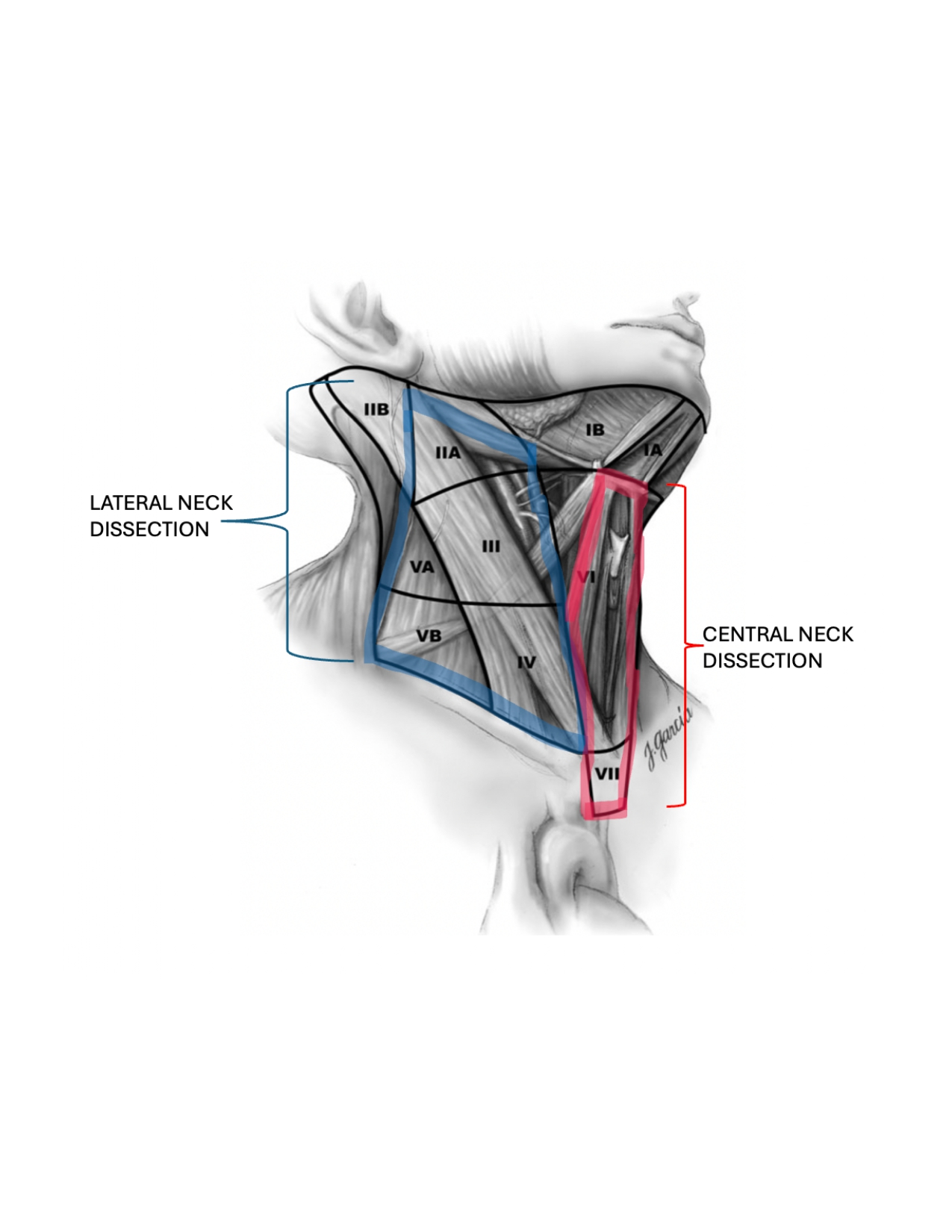
Image Source: Mary Ann Liebert, Inc.
If the cancer is grossly visible on imaging and/or objectively proven on biopsy, surgery to remove the cancer is the preferred treatment option.
Radioactive Iodine (RAI) is unlikely to be effective in patients who have grossly visible cancer on imaging.
~5% of all thyroid cancer patients (not just WDTC’s) have distant metastatic cancer discovered either at the time of cancer diagnosis or during surveillance.
Once the cancer has spread to a distant site, it is no longer curable.
Important to obtain gene sequencing and/or molecular analysis of the tumor cells to identify the DNA alteration driving the cancer.
Site of distant metastasis determines overall survival.
Treatment options
To explore these treatment options as a patient, you should be seen by a Head & Neck Cancer Oncologist who specializes in the treatment of advanced thyroid cancers (typically practicing at an academic university hospital).
If at any time the cancer is considered not curable, the patient / family / treatment team should collectively consider: