
The formation of the thyroid gland begins in the tongue (foramen cecum) when you are a fetus.
As a fetus develops, the thyroid travels down from the tongue, closely around the hyoid bone, along the midline front of the neck, to its eventual final location just above the chest plate.
The thyroglossal duct tract seals off shortly after the thyroid reaches its final destination.
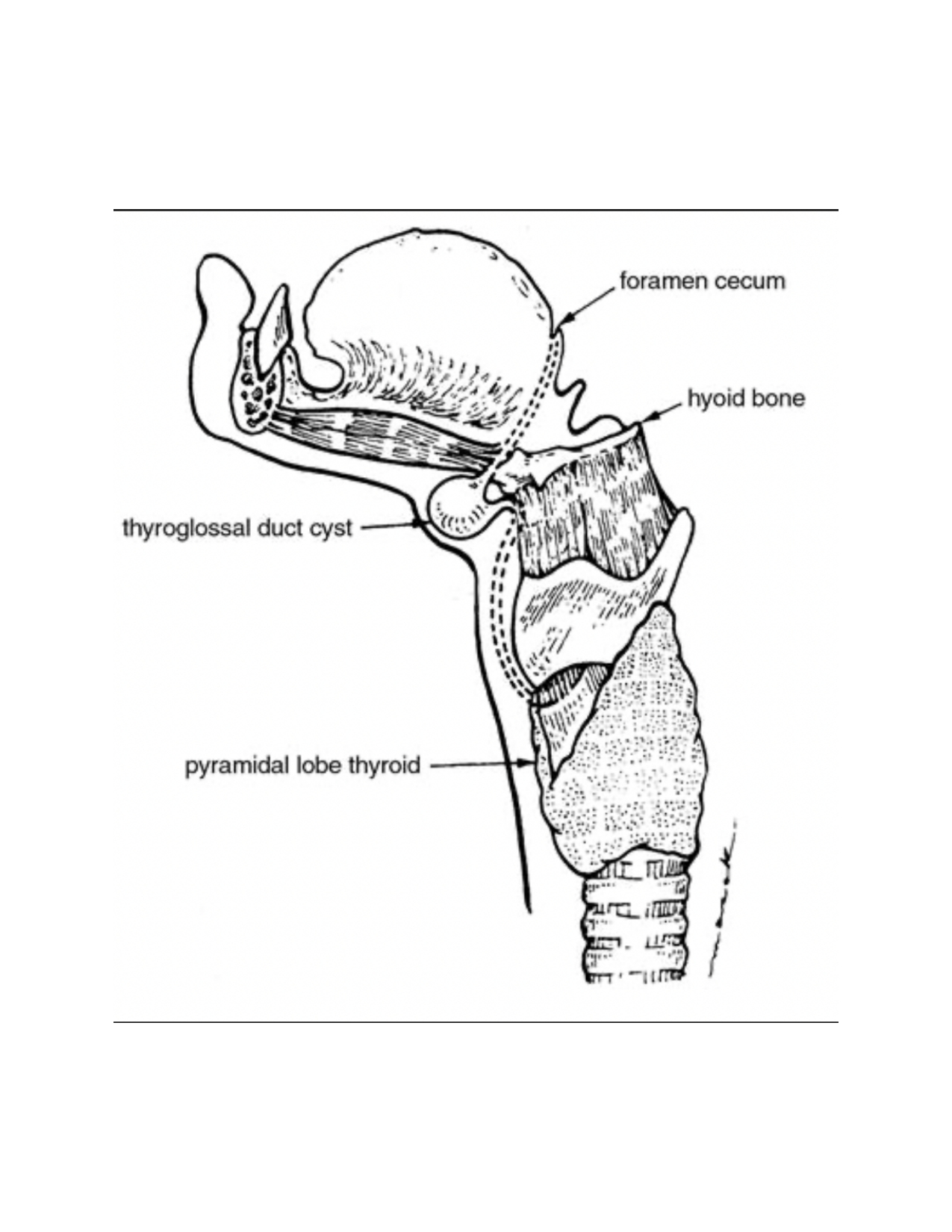
Image Source: Aleksey Dvorzhinskiy
TGDC’s most commonly present as an asymptomatic mass, just below the chin, in the midline of the neck.
On exam, a TGDC will rise in the neck when the patient sticks out their tongue.
Sometimes a TGDC can be infected causing severe swelling, pain, redness of the overlying skin, and rarely drainage of fluid from the skin.
When a TGDC is suspected on exam, an ultrasound of the neck should be obtained.
Observation
Ethanol ablation
Surgery to remove a TGDC should be considered when:
Surgery of choice is a Sistrunk procedure performed under general anesthesia.
Presence of functional thyroid tissue outside (ectopic) its normal expected location.
Imaging – depends on the location of the ectopic thyroid tissue:
Biopsy (FNA):
Observation
Surgery should be considered if: