
The thyroglossal duct cyst along with a small middle portion of the hyoid bone where the cyst often touches or wraps around.
Removing the cyst along with the hyoid bone is formally called a Sistrunk procedure.
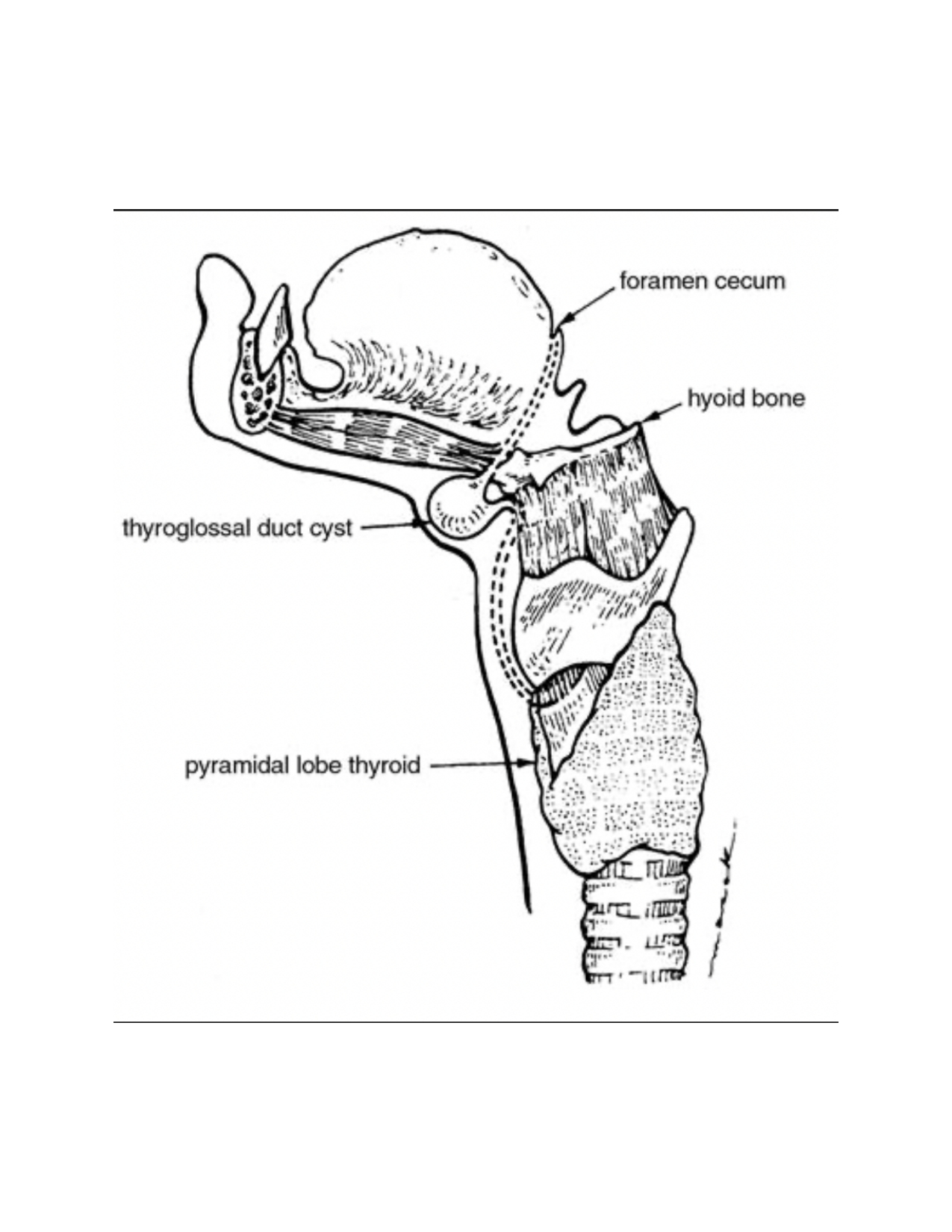
Image Source: Aleksey Dvorzhinskiy
Removing the bone along with the cyst greatly increases the ability to remove the entire cyst and therefore decreasing the risk of the cyst recurring and requiring revision surgery in the future.
There are no cosmetic or functional changes that you will notice after removing a small portion of the hyoid bone.
Biopsies are performed in order to rule out cancer.
Cancer of the thyroglossal glossal duct cyst is very rare (< 1% occurrence).
Given the risk for cancer is so low, biopsy is not necessary unless there are high risk features seen on imaging prior to surgery (solid portions, calcifications, irregular borders, etc.).
The surgery is performed under general anesthesia in the operating room.
General anesthesia involves receiving medication through an IV which causes you to go completely asleep, then a breathing tube is placed through your mouth and down your windpipe to help you breathe while you are asleep.
The breathing tube is removed before you wake up.
An incision is made in a natural horizontal crease of the skin closest to the location of the cyst, in the midline of the neck.
The incision needs to be long enough to remove the entire cyst (based on measurements made in a previous ultrasound or CT of the neck).
Surgery usually takes 45 – 60 minutes.
So long as there are no pain or nausea issues in the recovery area, most surgeries can be done as an ‘outpatient’ where you go home the same day.
It is not safe for you to drive home following general anesthesia.
Therefore, you should arrange for a ride to and from the hospital.
Typically the entire day lasts ~ 5 hours.
1 hour after surgery, you are transferred to your hospital room where your family and/or friends can see you.
The nursing staff takes care of you overnight.
Dr. Kay and his team see you the following morning and you are usually ready to be discharged home by 10:00 am provided your recovery is going as expected.
If for any unexpected reason you need to spend the night, your insurance company will pay for a 23-hour observation period at no extra cost to you.
Once the cyst is removed, there is a void (empty) space left in the neck which is at increased risk for filling with fluid (seroma) that can be uncomfortable and possibly lead to an infection.
To prevent against a seroma forming, either a pressure dressing will be wrapped around your head, or a small drain will be placed.
If you spend the night in the hospital, on most occasions the pressure dressing or drain can be removed the following day before you are discharged home.
Dr. Kay calls you with the pathology report 2-3 business days following the surgery.
When you schedule surgery, a post-operative appointment will also be scheduled for you ~ 6 weeks following your surgery.
You need a physical performed by your primary care provider to clear you prior to surgery.
If you see a sub-specialist for a significant medical issue like a cardiologist or pulmonologist, Dr. Kay will ask you to be cleared by this specialist as well.
If you are on a blood thinner, Dr. Kay will ask you to get permission to stop this blood thinner for the appropriate amount of time before surgery (varies by medication type) and for 5 days following surgery as well.
You can expect to experience pain and swelling around the incision lasting up to 1 week.
You can also expect to experience a sore throat and hoarse voice lasting up to 1 week.
You make experience some very mild restricted movement of the tongue when speaking and eating due to the scar tissue following surgery.
Everyone experiences pain in different ways and has different pain thresholds, therefore your experience may differ to some extent.
For 24 hours: Limit your activity for the first 24 hours following surgery and get plenty of rest as you recover from general anesthesia.
For 1 week: No heavy lifting or pushing (> 10lbs), active sports (e.g., running or jumping), strenuous exercise, heavy household work, or any activities that elevate your heart rate or blood pressure in order to reduce the risk of bleeding in your neck. Objects that cannot be lifted with one hand are considered too heavy.
There are no activity restrictions after 1 week.
In general, you may plan to return to work in 1 week, 2 weeks if your job requires manual labor, or as otherwise instructed.
Due to the sore throat caused by the breathing tube and surgical dissection, we recommend starting with liquids and soft foods.
You may progress to solid foods (your normal diet) as tolerated; this may take 1 – 3 days.
There are no restrictions in the positioning of your head and neck following surgery. You may relax and sleep in whatever position that is comfortable for you.
It is not uncommon for your sleep cycle to be affected by general anesthesia. Do your best to resume normal sleep patterns and avoid excessive daytime napping following the initial 24-hour rest period.
You can drive once you are off the strong (prescription) pain medication and when you can turn your head / neck to check your blind spots without hesitating. This may take 1-3 days.
Based on the risk for fluid developing under your incision, a pressure dressing was placed over the wound.
Please remove this dressing 24 hours after your surgery.
Use scissors to cute the gauze wrapping (careful not the cut the skin or hair) and remove all layers of gauze.
The last layer to be removed will be a small rectangular shaped wax coated piece of gauze.
Please record your drain output twice daily.
OK to get the drain wet in the shower.
Dr. Kay’s office will call to arrange drain removal 1-2 days following your surgery.
Your incision was closed in two layers:
You may bathe or shower as soon as you like after surgery.
If the glue and bandage is still present 2 weeks after surgery, you may peel off the bandage (Steri-Strip) and the rest of the glue.
After the bandage comes off, you may notice several small bumps under the skin along your incision line and the incision line may appear raised.
As your incision heals, it is not uncommon to experience sensations of tingling, burning, itching, or pinching / shooting pains.
Once the bandage is off, please purchase over the counter Vitamin E oil from a pharmacy or supermarket (Vitamin E oil capsule which can be broken open are an acceptable alternative).
Once the bandage is off, please keep your incision out of direct sunshine for the first 3 months after surgery (using shade, a scarf, and/or sunscreen with SUV 30 or higher with both UVA and UVB protection) in order to prevent discoloration of the scar.
Ice compresses can help to treat swelling and pain around the incision. Apply for 10 min at a time. You can repeat every 30 minutes as needed.
Sore throat lozenges (particularly those with the active ingredient ‘Benzocaine’ such as found in Cepacol lozenges) will help to treat the discomfort deep in your throat.
Drinking fluids frequently will help the small scratches inside the throat caused by the breathing tube to heal more quickly and also relieve your pain faster.
Over the counter Tylenol (acetaminophen) can be taken every 6 hours as needed for pain relief, up to 1,000 mg each dose, do not exceed 4,000 mg total in 24 hours. Do not take 3,000 mg total per day for > 3 consecutive days.
Over the counter NSAID’s (Non-Steroidal Anti-Inflammatory Drugs)
OR
In situations when the above pain control regimen does not control your pain symptoms adequately, you were prescribed 5 tablets of a low dose narcotic medication (either Tramadol or Hydrocodone / Acetaminophen).
If you are discharged home on the same day of surgery, you will be given an antinausea prescription called Zofran (ondansetron). This comes in a tablet form that dissolves underneath your tongue.
You can use this as needed if you are experiencing nausea. Please have a low threshold to use this in order to prevent vomiting (which can increase the risk of bleeding in your neck).
You will receive narcotics as part of your general anesthesia on the day of surgery and you may also take a prescription narcotic pain medication following surgery. These narcotic medications can cause constipation.
In order to prevent this, you may consider purchasing an over-the-counter stool softener (such as docusate or senna) and take for 24-48 hours following surgery as directed on the package (especially if you are prone to constipation).
You should resume taking all other medications the day after surgery, unless instructed otherwise by your primary care provider.
If you were on any blood thinners (Plavix, Coumadin, Eliquis, Xarelto, Aspirin, etc.) prior to surgery, please do no restart the medication until 5 days after your surgery to limit the risk of bleeding, unless instructed otherwise.
Due to the effects of the breathing tube being placed during surgery, you may experience thick mucus in your throat for 24-48 hours. It is ok to gently clear your throat and cough to clear this mucous.
If the sensation of mucous in your throat persists for > 48 hours, it is usually not because there is still mucous there. At this point, persistent inflammation and sensitivity of the vocal cords caused by the breathing tube can mimic the sensation of mucous and is best treated by drinking plenty of liquids, using over the counter throat lozenges with the active ingredient ‘Benzocaine’ such as found in Cepacol lozenges, and avoiding further throat clearing / coughing.
Swelling beneath or near your incision site, particularly if it is visibly noticeable and/or causing pressure in the neck.
If you notice rapid and progressive swelling in your neck, or bleeding from your incision, please call 911 as this could represent a hematoma, or active bleeding in the neck, and this is a medical emergency.
If you notice redness and itching around the bandage, especially if starting 24-48 hours after surgery, you may be experiencing an allergic reaction to the skin glue or the white steri-strip bandages.
When surgery is scheduled, an appointment should have been made for you to follow-up ~ 6 weeks after surgery.

Specific to excision of a thyroglossal duct cyst:


Pain following surgery typically lasts up to 5-7 days and is usually tolerated with little to no narcotic use (see more information in the ‘What to Expect Following Surgery’ section).
There is very low risk (~1 %) for infection following hemithyroidectomy.
Antibiotics are given to you during surgery, but none are routinely used following surgery.
There is a 1% chance of significant bleeding following surgery.
Signs of bleeding include significant swelling in the front of the neck, similar to the appearance of a bullfrog.
Sometimes this bleeding stops on its own, other times it does not and it can be life threatening requiring urgent surgery to stop the bleeding.
Risks for bleeding are higher when a patient cannot be taken off their blood thinners completely.
You are required to be cleared by your primary care provider prior to surgery and any other sub-specialty providers who provide care for important medical conditions.
The incision is made as small as possible (based on thyroid lobe size and the patient’s anatomy) and attempted to be hidden in a natural skin crease (if present) or hollow of the neck.
Ultimately it is up to how your body heals (based on previous incisions or scar).
Typically, incisions in the neck heal very nicely.
If there is a history of keloid formation, a steroid called Kenalog may be injected into the skin at the time of surgery to lower the risk of keloid formation as best as possible.