
Hyperthyroidism
Background on Thyroid Function
- The purpose of the thyroid gland is to produce thyroid hormone which is released into the blood and then circulates throughout the body.
- Thyroid hormone helps to control metabolism, effects growth and development, controls body temperature, and helps to regulate the cardiovascular system among many other important functions in the body.
- There are two forms of the hormone that are produced: T4 (thyroxine) and T3 (triiodothyronine), accounting for 80% and 20% of hormone in the blood respectively.
- The production of thyroid hormone is controlled by the brain (specifically the pituitary gland).
- The brain continuously measures thyroid hormone levels in the blood, and produces a hormone called TSH (thyroid stimulating hormone or thyrotropin) when more thyroid hormone is needed.
- Levels of TSH and T4 / T3 in the blood have an inverse relationship, or teeter totter effect:
- When T4 and T3 levels go down, TSH levels will go up to compensate, and vice versa.
- This is a tightly regulated feedback loop (or hormone axis in the body).
Hyperthyroidism
- Diagnosis:
- Overt hyperthyroidism (aka thyrotoxicosis) is defined by elevated free T4 and total T3, with low TSH levels in the blood.
- Subclinical hyperthyroidism is defined by high-normal free T4 and total T3, with a low TSH.
- TSH level measurements can be affected by biotin supplements (commonly present in hair and nail supplements), and therefore these supplements should be stopped 1 week prior to blood draw.
- Symptoms include:
- Unexplained weight loss, rapid/irregular heartbeat, tremor, sweating, irritability, heat intolerance, insomnia, diarrhea, nervousness, anxiety.
- Goiter formation causing compressive symptoms (constant pressure in the neck, choking sensation, difficulty swallowing or breathing, stridor).
- Long-term consequence of untreated Hyperthyroidism:
- Weight loss, osteoporosis (progressive bone thinning), atrial fibrillation (uncontrolled fast heart arrythmia), blood clots, muscle weakness, tremor, neuropsychiatric symptoms (anxiety, depression), rare cardiovascular collapse and death.
Graves’ Disease.
- Syndrome of hyperthyroidism, goiter (enlarged thyroid gland), ophthalmopathy or exophthalmos (bulging eyes or Thyroid Eye Disease), and dermopathy (pretibial myxedema – swelling and discoloration of the lower leg skin).
- Considered an auto-immune disease where the body’s immune system attacks the thyroid, mistaking it for something foreign to the body.
- Antibodies are made specifically to attack the thyrotropin (TSH) receptor, referred to as Thyrotropin Receptor Antibodies (TRAb).
- Antibodies attacking this receptor stimulate thyroid hormone production and release into the blood independent of TSH levels made by the pituitary gland.
- Disrupts the normal tightly regulated feedback loop.
- Can also cause the thyroid gland to grow and form a goiter.
- Most common cause of hyperthyroidism in the U.S.
- More common in ages < 45.
- Can resolve in 30% of patients spontaneously or with medical treatment.
- Diagnosis:
- Diffuse intense uptake on thyroid uptake scan.
- Elevated Thyrotropin Receptor Antibody (TRAb) and Thyroid Stimulating Immunoglobulin (TSI).
- Exam with diffuse bilateral goiter formation.
- Exam with bulging eyes (orbitopathy).
Toxic thyroid nodule vs Toxic multinodular goiter.
- Caused by a single nodule or multiple nodules autonomously producing thyroid hormone independent of Pituitary Gland feedback mechanism and TSH levels.
- Thought to be caused by somatic (non-inherited) activating mutations of DNA genes regulating thyroid growth and hormone production.
- More common in ages > 45.
- More common in regions of iodine deficiency.
- Usually progressively worsens overtime and less likely to resolve spontaneously or with medical treatment.
- Diagnosis:
- Focal uptake in one or more discrete regions on thyroid uptake scan.
- Focal uptake corresponds to a discrete nodule on ultrasound.
Other rare causes for Hyperthyroidism.
- Familial non-autoimmune hyperthyroidism (genetically inherited).
- Amiodarone (prescription medicine used to treat heart arrythmias) induced thyrotoxicosis (5-10% of amiodarone patients).
Causes for temporary hyperthyroidism:
- Subacute thyroiditis.
- Inflammation (thought to be due to a virus) which causes release of stored thyroid hormone.
- Typically followed by a period of hypothyroid symptoms until thyroid hormone stores can be replenished.
- Can present with or without localized pain in the thyroid and/or fever.
- Thyroid Antibody levels and Thyroid Uptake Scan will both be normal.
- Post-partum thyroiditis.
- Brief episode of thyroid inflammation and release of thyroid hormone following delivery.
- Also typically followed by a period of hypothyroid symptoms until thyroid hormone stores can be replenished.
- Thyroid Antibody levels and Thyroid Uptake Scan will both be normal.
Labs
- In addition to TSH, free T4, and total T3:
- Thyrotropin Receptor Antibody (TRAb) and Thyroid Stimulating Immunoglobulin (TSI) can be measured in the blood.
- Should be elevated in Graves’ Disease but not in a toxic nodule or toxic multinodular goiter.
Imaging
- Radioiodine scan (‘thyroid uptake scan’).
- A low dose radioactive iodine (typically I-123) material is ingested via pill or fluid.
- This material is absorbed by overactive thyroid cells and is visible on special cameras taking pictures of the thyroid.
- Different patterns of iodine uptake will help differentiate between the possible causes of hyperthyroidism.
- A single toxic (or ‘hot’) nodule with be visible as focal uptake in one discrete area of the thyroid.
- It is very rare for hot thyroid nodules to be cancerous.
- Hot nodules therefore do not need to be biopsied (aka FNA) unless there are high risk features present on ultrasound.
- Multiple toxic (or ‘hot) nodules will be visible as focal uptake in multiple discrete areas of the thyroid.
- Presence of a hot nodule(s) should be confirmed with a discrete visible nodule on ultrasound in the same location.
- Diffuse uptake in both lobes of the thyroid is diagnostic of Graves’ disease.
- There should be no uptake if hyperthyroidism is temporary in nature:
- Subacute, post-partum thyroiditis, or amiodarone induced.
- Should be avoided in pregnant and breastfeeding patients.
- Can result in cretenism of the baby (complete loss of thyroid function).
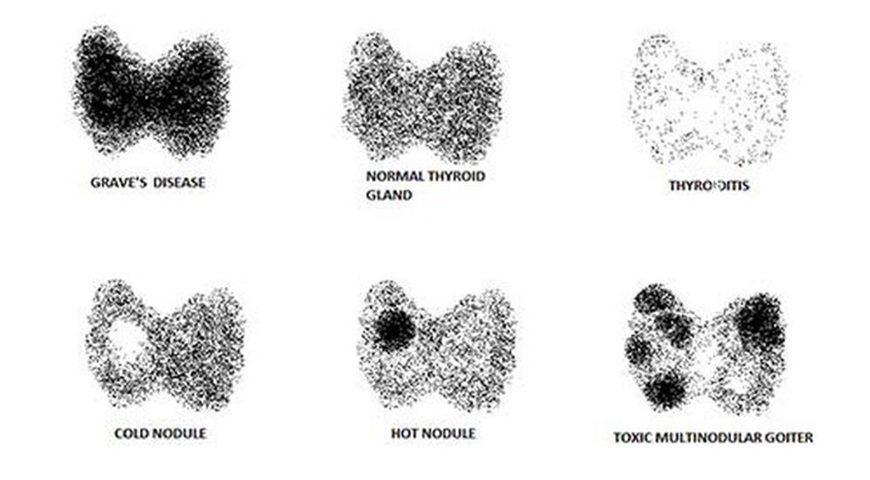
Image Source: Medizzy
Ultrasound
- Should be obtained if:
- Toxic nodule(s) discovered on Thyroid Uptake Scan to correlate location for possible surgery.
- Graves’ Disease is diagnosed and surgery is being considered as a treatment option.
- Helps in surgical planning and anticipating the size of incision needed.
- Goiter (enlarged thyroid) is felt on exam.
To learn more about Hyperthyroidism
To learn more about the Thyroid, head back to the Thyroid main page here.
Schedule your consultation today
For Personalized and Expert Surgical Treatment
of Your Thyroid and Parathyroid
